Most of operations I have ever taken over have already been looked at by someone. Reports existed. Recommendations had been made. In most cases the advice was reasonable. In most cases it had not worked, because it had been aimed at the wrong thing.
At a broadband start-up where I built the service operation from scratch, the inherited assumption was that delivery failures were a training problem. They were not. The processes themselves had never been designed for the volume the business was now handling. At a major programme where I led a transformation across a £200m operation, the presenting issue was cost. The actual constraint was how authority had been distributed: responsibility had been pushed down, but the matching authority had not followed it. Every process improvement attempted before that structural fault was addressed had been undermined by it.
The pattern repeated at every scale. At a network operator preparing for a merger, on-the-day delivery was failing on roughly one in eight jobs. The assumption had been that the team needed tighter standards and motivation. The real problem was that every process and quality gate had been built piecemeal and never redesigned as a coherent system.
In each case, the fix started with finding the actual constraint, not the most visible symptom. That principle, learned across fifteen years of leading operations, is why my practice is built the way it is.
The problem with recommendation-first advisory
Most advisory engagements follow a familiar sequence. An advisor arrives, spends time with the leadership team, reviews data, and produces a set of recommendations. The advisor presents them, then leaves. The client is left to implement.
The sequence sounds logical. The flaw is in the starting point. The recommendations are shaped by what the advisor sees in the time available, filtered through whatever framework they brought with them. If the framework emphasises financial performance, the recommendations will focus on cost and margin. If the framework emphasises culture, the recommendations will focus on people and communication. The actual constraint may sit in neither place.
I have inherited the output of recommendation-first engagements more than once. The common pattern is that the recommendations address the symptoms the leadership team described in interviews, not the structural fault underneath. A business whose meetings produce no decisions will be told to improve its meeting discipline. The actual problem may be that authority has never been clearly assigned, so nobody in the room has the mandate to decide. Fixing the meetings changes nothing. Fixing the authority structure changes everything.
The pattern is consistent: when you start with a recommendation, you commit resources to fixing what you think is broken. When you start with a diagnostic, you find out what is actually broken before you commit anything. The difference in cost, time, and outcome is substantial.
How the diagnostic-first principle works in practice
Every engagement in my practice begins with one of two diagnostics, depending on whether the client is an organisation or an individual.
For organisations, the entry point is the Invincibility Blueprint. This is a structured assessment that examines how the business actually operates: where decisions are made, how authority flows, what the management cadence looks like, where execution breaks down, what the data says about performance versus what the leadership team believes. It produces a findings report, a maturity scorecard, and a prioritised set of actions. Two routes exist: one where I lead the diagnostic directly, and one where the client’s team completes structured assessments and the analysis is processed through purpose-built diagnostic engines before I review and interpret the results.
The individual equivalent is the Individual Invincibility Blueprint. This is a management competency assessment that maps capability across 22 axes, from delegation and control through to authority, decision-making under uncertainty, and the ability to build high-performing teams. It does not test knowledge. It examines how the person actually manages: what they do when they delegate, how they follow up, how they handle resistance, how they set and enforce standards.
Both diagnostics serve the same function. They establish where the real constraint sits before anyone decides what to do about it.
What happens after the diagnostic
This is where the practice architecture earns its design. The diagnostic does not simply produce a report and hand it over. It determines which path the engagement takes next.
An organisation whose Blueprint reveals that competitive positioning is unclear or that the marketing function is operating on instinct rather than evidence may need a structured Marketing Strategy Plan before any operational transformation begins. An organisation whose constraint is in how the business is run day to day may need embedded transformation: someone senior enough to take ownership of the change and stay long enough for the new operating disciplines to hold. A business preparing for sale needs a different intervention entirely, focused on packaging operational evidence for due diligence and strengthening the areas acquirers will test.
For individuals, the assessment may reveal that 1:1 leadership development is the right path, or that a team needs group training to build shared management capability, or that the leader needs ongoing strategic oversight rather than a defined programme.
The routing follows from evidence, not from what happens to be on the advisor’s menu. A practice built this way does not need to sell every client the same thing. The diagnostic tells both of us which path makes sense, and which paths would be a waste of time and money.
Why the infrastructure underneath matters
One question I hear from people reviewing my practice for the first time is how a sole advisor delivers diagnostic depth at this level without a large team behind them. The answer is that I have spent the past year designing and building five purpose-built diagnostic engines that sit underneath the entire practice.
These are not off-the-shelf AI tools or questionnaire platforms. Each engine encodes the frameworks, quality standards, and pattern recognition I have developed across fifteen years of operational leadership. They process evidence, identify system-level stress points, and surface the decisions that matter, before I review, interpret, and act on the results.
The engines cover organisational diagnostics, marketing strategy, management competency assessment, operating system design, and goal-to-calendar decomposition. They are the reason a single senior advisor can deliver the analytical rigour that would normally require a team, at a pace and price point that makes sense for businesses between £10m and £200m in turnover, the segment the large firms have never served well and the sole practitioners have never had the infrastructure to serve properly.
Diagnostic depth, in this model, is not a function of team size. It is a function of how the practice was built.
What to look for if you are evaluating advisory
If you are a CEO, MD, or operations director considering an external advisor, the diagnostic question is worth asking before you sign anything. Three things to look for:
Does the advisor start by understanding your specific constraint, or do they arrive with a pre-formed view of what needs fixing? The pre-formed view may be right. But you are paying for accuracy, and accuracy comes from diagnosis, not assumption.
Will the engagement structure follow from the diagnostic findings, or is it a fixed programme regardless of what the assessment reveals? Fixed programmes serve the advisor’s delivery model. Diagnostic-first structures serve the client’s actual situation.
Is the advisor going to stay long enough for the changes to hold, or will they produce a report and leave you to implement? The gap between recommendation and implementation is where most advisory value is lost.
These are not abstract questions. They determine whether the advisory spend produces a return or produces a shelf of documents.
The architecture is the answer
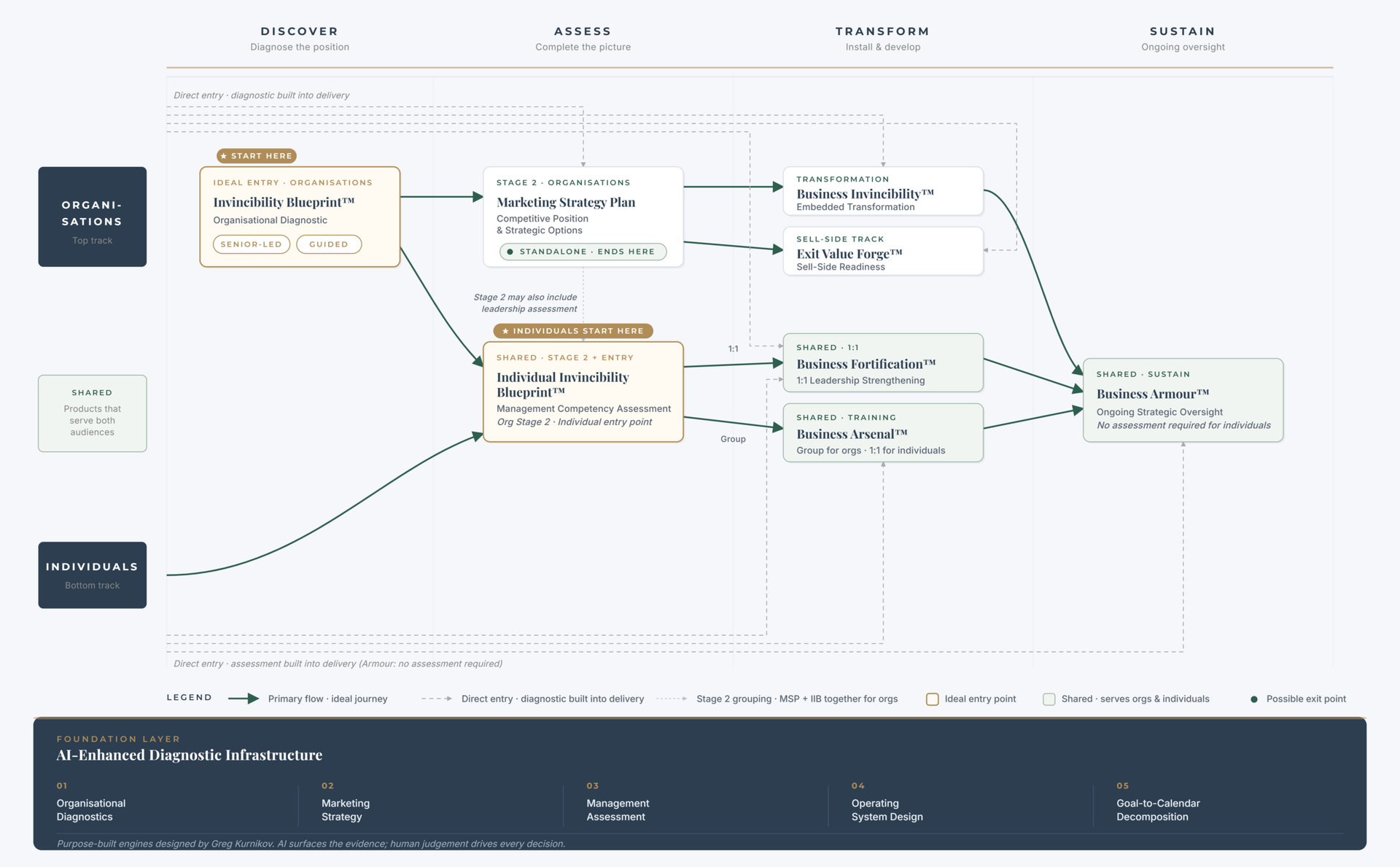
I built my practice around a single conviction: that the most expensive mistake in advisory is acting before you understand. Every service I offer, for organisations and for individuals, flows from a diagnostic that establishes where the real constraint sits. The structure exists so that no client pays for an intervention they do not need, and every intervention addresses the problem that actually matters.
The product flow diagram that accompanies this article shows the architecture. Two tracks. Four shared products. Five diagnostic engines underneath. Everything flows from left to right: discover, assess, transform, sustain. The entry point is always the same. What follows depends on what the evidence says.